
Max Hospital, Patparganj, New Delhi
Elevate Health Solutions, Rajouri Garden, New Delhi
Max Hospital, Vaishali, Ghaziabad
Max Hospital, Patparganj, New Delhi
Elevate Health Solutions, Rajouri Garden, New Delhi
Max Hospital, Vaishali, Ghaziabad

27 May, 2023
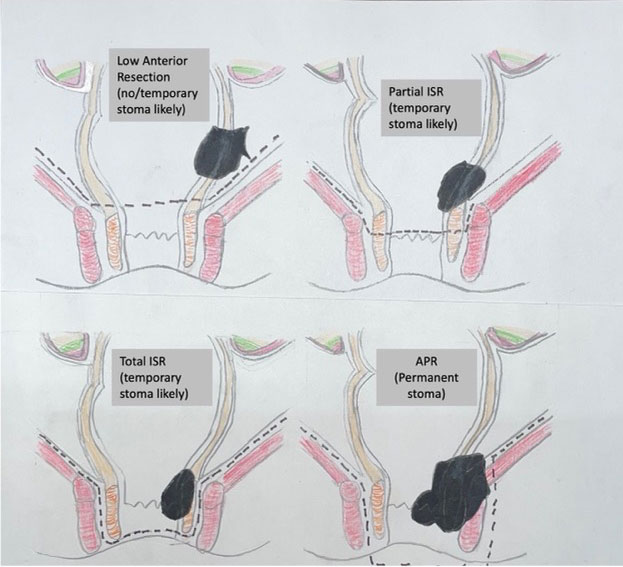
The biggest question in a patient’s mind and treating surgical team when dealing with distal rectal cancer (cancer in the distal most part of digestive system) is whether sphincter preservation (or simply restoration of normal passage for stools) is possible with good functional and oncologic outcomes or not. Distance of the tumour from the anal verge, is an important determinant of ability to achieve this (farther the tumour from the anal verge, the more the chances). Equally important are several other considerations such as extent of involvement of rectal wall, type of tumour (polyp, cancer and predicted biologic behavior of cancer), patient’s age, strength of sphincter muscle, and continence besides technical expertise of the treating rectal cancer surgeon. This ability is considerably enhanced by appropriate use of radiotherapy/chemotherapy tailored to patient’s condition and tumour characteristics prior to surgery. Distal rectal cancer presents technical challenges at surgery in view of the narrow space and a complex sphincter anatomy and mechanism sometimes resulting in need for specialized technique of Intersphincteric resection (ISR) in which dissection is done between the external and internal part of the sphincter muscle to ensure complete tumour removal as well as preservation of continence mechanism and a part or the entire internal sphincter is removed with tumour.
Careful and detailed evaluation of patients by colorectal cancer specialist is needed while considering (sphincter saving) rectal cancer surgery. These considerations include:
This surgery can be done well both laparoscopically as well as by use of robotic technology thereby resulting in lesser pain and faster recovery. Like all surgical procedures, this surgery can be also be associated with some risks which the treating team would usually explain to the patient and family. Creating a temporary diverting ileostomy at the time of the first surgery (ISR) gives time for healing to take place. This ileostomy would be closed once the treating team has ensured that good healing has occurred at the site where the colon was joined to the anal canal. Despite best efforts, some patients in whom this procedure is planned, patient may need a permanent stoma (colostomy) the need for which may sometimes arise during the planned sphincter saving procedure or sometimes later. At the same time, it is important to understand that it is extremely important that aggressive attempts at sphincter salvage or sparing should not compromise complete cancer removal and performing a surgery called APR (entailing creating a permanent passage of stools on the abdomen called colostomy) may be sometimes in patient’s best interest. Incomplete removal will not only lead to a very poor outcome in terms of survival and pain but also lead to poor functional outcomes or need for permanent stoma later. In appropriately selected patients undergoing ISR, complete tumour removal can be removed and at the same time the preserved external sphincter ensures good continence in absence of previous surgery in that region provided the sphincter muscle has good strength which would usually have been assessed carefully prior to surgery. Although, there is initially increased stool frequency, urgency, and occasional incontinence, this usually settles over time and the long-term outcomes are usually good provided the patients are deemed good candidates for this procedure after a careful and detailed evaluation.
Click on to see a story of successful sphincter salvage done (https://www.drvivekmangla.com/video.html) in a middle-aged lady from Himachal Pradesh diagnosed with distal rectal cancer about 3.5 cm from anal verge who travelled all the way for this treatment with us with good outcomes. She was initially treated with chemoradiation followed by a specialized surgical technique called laparoscopic intersphincteric resection.
To learn more about sphincter saving in distal rectal cancer and avoiding permanent colostomy in distal rectal cancer, please click on https://youtu.be/ZMfRdJ0JYVs

Room No. 2623, 6th Floor, Tower 2

Mon to Sat: 02:00 pm-05:00 pm
Room No. 2014, Ground Floor, West Wing

Mon to Sat : 8:30am - 9:00am, 6:00pm-7:00pm
E29B, Ground Floor, E Block, Rajouri Garden, New Delhi-i 110027
Mon to Sat : 7:30-8:30 am, 7:30 -8:30 pm

